
Apicoectomy #46 (30) on Bisphosphonates
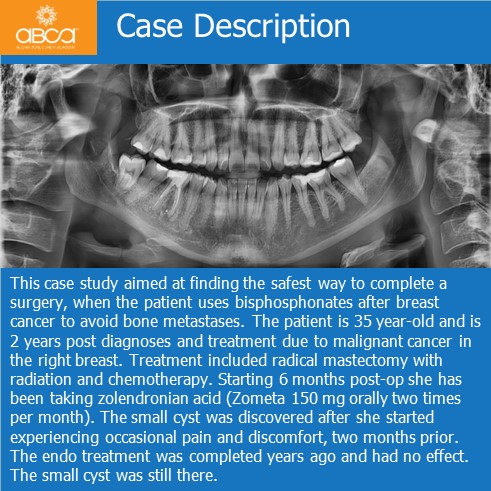
This case study aimed at finding the safest way to complete a surgery, when the patient uses bisphosphonates after breast cancer to avoid bone metastases. The patient is 35 year-old and is 2 years post diagnoses and treatment due to malignant cancer in the right breast. Treatment included radical mastectomy with radiation and chemotherapy. Starting 6 months post-op she has been taking zolendronian acid (Zometa 150 mg orally two times per month). The small cyst was discovered after she started experiencing occasional pain and discomfort, two months prior. The endo treatment was completed years ago and had no effect. The small cyst was still there.
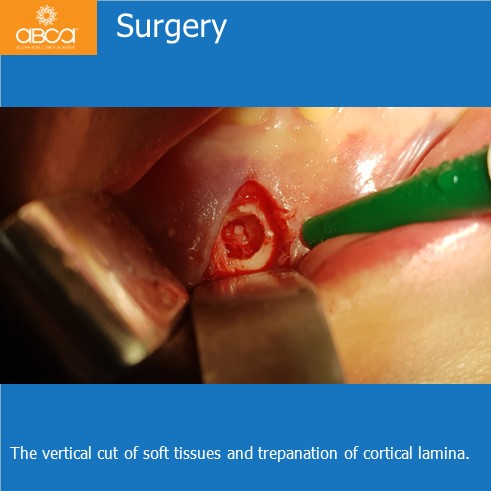
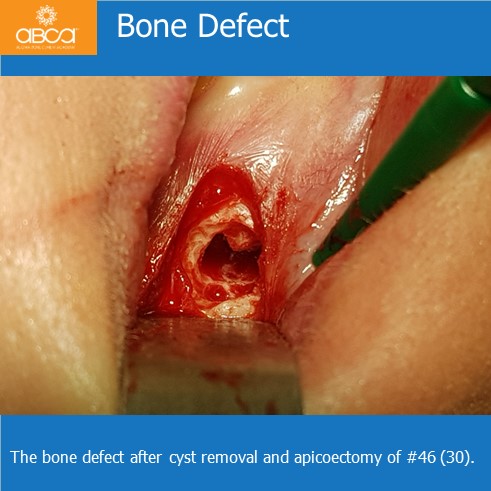
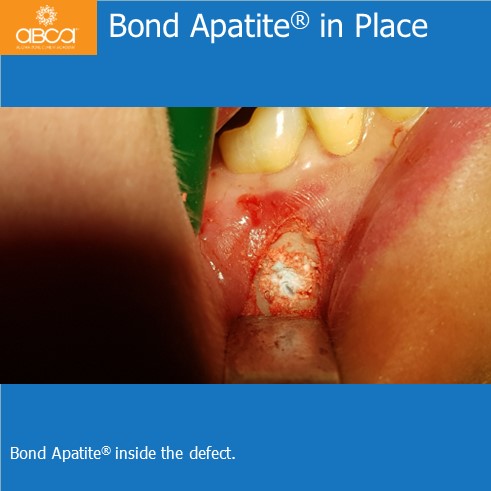
To minimalize the risk of BRONJ (Bisphosphonate Related Osteonecrosis of the Jaws) the patient underwent pre-op treatment. CTX blood examination was used to calculate the risk level, Amoxicillin was prescribed two days before operation, and continued for 7 days. A mesial root resection was performed on tooth #46 (30) using small vertical soft tissue cuts, recommended for a small inflammatory lesion up to diameter about 6-7 mm. Preparation of the root canal is performed with backfill with MTA, cyst removal with histopathology examination that confirmed a radicular cysts without no symptoms of BRONJ. The bone defect is filled with Bond Apatite®. 3 and 6 month follow-up images show good remodelling of the bone, and healing was observed.
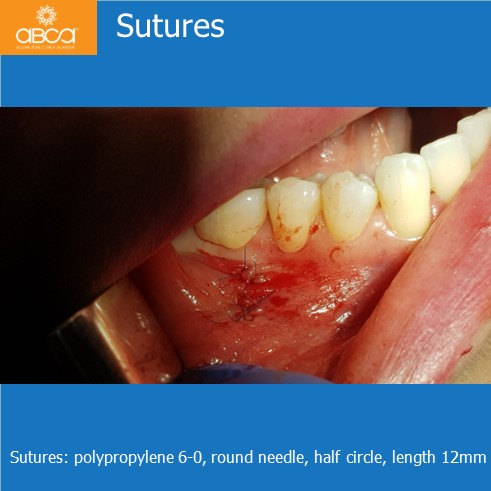
The vertical cut makes it easier to minimalize the risk of BRONJ and to suture. In addition, no secondary BRONJ inflammatory reaction was observed. The conclusion is that the minimal invasive microsurgery and filling of the bone defect with Bond Apatite® under bisphosphonate treatment, is safer than extraction without bone defect filling.





![]()
![]()
![]()